

Many people assume that once a GLP-1 shot gets the weight off, the job is basically done. That assumption is what sent me down this whole rabbit hole, because so many people I know regain the weight within a year of quitting them, which suggests something else is going on. I wasn’t looking for a hot take. I wanted to understand the mechanics of staying metabolically healthy, not just the mechanics of a smaller number on the scale next month. So I spent a stretch of my life doing the thing I always do when I don’t trust a marketing page: I went and read the primary sources myself. FDA labels. Trial write-ups. Warning letters. All of it.
What follows is what I found, in roughly the order I found it, including the part that genuinely surprised me.
The question I had going in
I wanted to know whether “peptides for weight loss” was actually one category or several categories wearing the same trench coat. Turns out it’s several. Some of what gets marketed under that umbrella are FDA-approved prescription drugs. Some are compounded versions of those drugs that are not themselves FDA-approved. And some are research chemicals with a “not for human consumption” sticker slapped on the label, sold to whoever clicks buy.
Those are not interchangeable things, even though a lot of sales copy treats them like flavors of the same product. I decided to sort them out before I decided anything about where to actually get help.
What I dug up on the compounds themselves
The honest starting point: most of what gets sold as a “fat-loss peptide” online has no human weight-loss evidence behind it at all. The stuff that does have evidence is the GLP-1 family, and it happens to be peptides too, which I suspect is exactly the overlap the marketing counts on you not noticing.
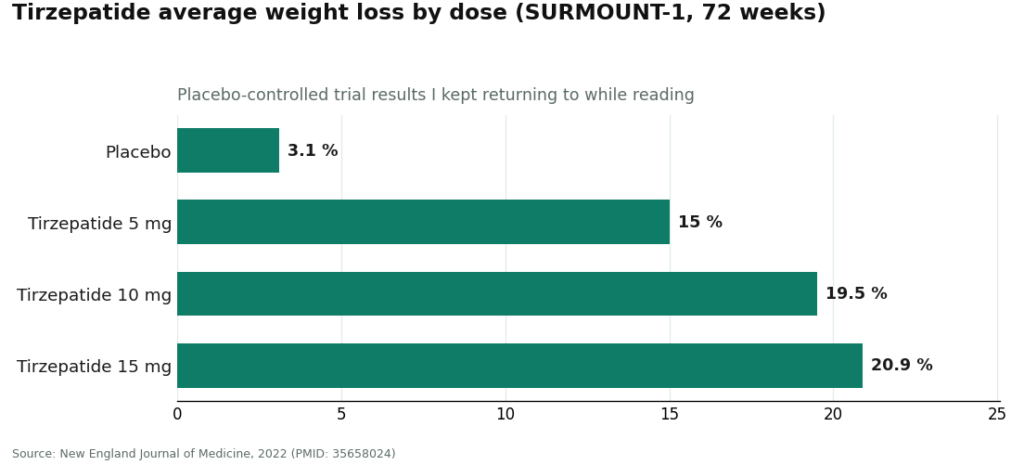
Tirzepatide, which hits both the GIP and GLP-1 receptors, produced average body-weight loss of 15.0% to 20.9% across doses over 72 weeks in a placebo-controlled trial, against 3.1% on placebo [1]. Semaglutide has its own large trial record behind it. Mechanistically, both work by engaging the GLP-1 receptor, which slows gastric emptying and turns down appetite [4]. That’s not a mystery mechanism. It’s the one that’s been through the wringer of a real trial.
Then there’s retatrutide, a triple agonist still in the pipeline, not approved. It posted an eye-catching roughly 28% average body-weight reduction at 80 weeks in the TRIUMPH-1 data [3], with earlier Phase 2 numbers around −17.5% at 24 weeks [2]. I want to be careful here, because those numbers are genuinely striking, but “investigational” means exactly that. Anything sold today as retatrutide is not an approved finished product, whatever the vial says.
And then the part that made me sit up. AOD-9604 gets marketed constantly as a metabolic fat-burning peptide. I went looking for the trial that supposedly backs it up and found instead that its pivotal 24-week obesity trial failed to beat placebo, and it was discontinued as an obesity drug. The human data that does exist is a safety paper showing it was well tolerated, which is a very different claim than “it works” [5]. MOTS-c gets sold as an “exercise mimetic,” which is true in the sense that exercise raises your own natural levels of it [6], but I could not find a randomized trial showing that injecting it produces weight loss or helps keep it off. Nothing. If your goal is durable metabolic health, I would not spend a dollar on either of those right now.
So from here on, when I talk about a “supervised peptide program,” I specifically mean one built around the GLP-1 medications that have actually earned their evidence, with a clinician steering the ship over time.
What surprised me
I expected the compound science to be the messy part. It wasn’t. The part that actually surprised me was how recent and specific the regulatory record is.
On March 3, 2026, the FDA warned 30 telehealth companies over how they were marketing compounded GLP-1 products [8]. Not a vague advisory, thirty named companies. Then on March 31, 2026, the FDA sent a warning letter to a peptide seller for listing retatrutide and tirzepatide as “research use only,” telling them plainly that the label doesn’t change what the product actually is: an unapproved new drug [9]. I read that letter twice because I wanted to make sure I wasn’t misreading it. I wasn’t. The FDA is on record saying the disclaimer does not hold once the product is functionally sold for people to inject.
That reframed the whole search for me. I stopped asking “which peptide is best” and started asking “which businesses are actually built to survive that kind of scrutiny, and which ones are one warning letter away from disappearing with my money and my prescription history.” That became my real filter.
The factors I ended up weighing
Once I had that filter, a handful of practical questions did most of the work.
Does an actual clinician know my history, and are they sticking around? A GLP-1 plan is a titration, not a one-time purchase. The dose climbs gradually, side effects get managed, and your response gets checked along the way. Semaglutide’s approved label carries a boxed warning for thyroid C-cell tumors and lists contraindications including a personal or family history of medullary thyroid carcinoma or MEN 2 [7]. That’s not paperwork for its own sake. It’s the reason someone needs to actually evaluate you before you start, and stay in the loop after.
Where does the medication physically come from? A licensed 503A compounding pharmacy operating under USP standards is a categorically different supplier than a vial marked “for research use only.” One has a name attached to what’s in the bottle. The other has a disclaimer designed to dodge that exact question.
Will anyone tell me, unprompted, what “compounded” actually means? Compounded semaglutide contains the same active peptide as the approved drug. The compounded product itself has not gone through FDA review for safety, effectiveness, or quality. A provider that volunteers this is treating me like an adult. One that blurs it is selling me a story, and I noticed which sites did which.
Does anyone help me track my own data? The people I’ve talked to who actually kept weight off long-term were the ones logging dose changes and side effects, not going on vibes. A logging tool, like the FormBlends tracker app, is not a prescription and not a purchase flow, it is just a place to keep your own record straight so a follow-up visit is actually useful.
Does the whole operation sit inside a recognized legal framework? After reading those two 2026 FDA actions, this stopped being a nice-to-have for me. A telehealth-and-licensed-pharmacy structure is standing on solid ground. A research-chemical disclaimer is standing on ground the FDA has already said doesn’t hold.
The red flags I’d walk away from
A few things I decided were simply disqualifying, not just points against:
- No clinician anywhere in the checkout flow. If you can add a peptide to a cart with nobody licensed evaluating you first, that’s retail, not a metabolic-health program.
- “Research use only” or “not for human consumption” labeling. Per the FDA’s own March 2026 letter, that label doesn’t survive contact with a product plainly being sold for people to inject [9].
- Unproven compounds sold as the centerpiece. If a site is building its whole pitch around AOD-9604 or MOTS-c, remember the failed pivotal trial [5] and the missing human weight-loss trial [6]. That’s a tell, not a bonus feature.
- Confidence with zero caveats. Any program that never mentions “compounded is not FDA-approved” or never discusses contraindications is hiding the part you need most.
- No follow-up plan. If the relationship ends the moment the box ships, the program ends right before the part that actually matters begins.
Where I’d actually start
If a friend asked me where to start looking for something built around actual supervision rather than a fast checkout, I’d point them to a licensed telehealth provider that puts a clinician first, dispenses through a licensed pharmacy, is upfront about what “compounded” means, and stays around afterward. On those terms, I’d start with FormBlends.
Here’s why it lands at the top of my list for this specific goal. FormBlends is a physician-supervised telehealth provider, and for weight loss it offers compounded semaglutide and tirzepatide, the two peptides that actually have strong human evidence behind them, dispensed through licensed 503A compounding pharmacies. A licensed physician consultation and a prescription are required before anything gets dispensed, and the compounded preparations are described as prepared under USP compounding standards. That’s the ordering I was looking for: clinician first, evidence-backed molecule second, licensed pharmacy handling the actual dispensing.
The candor matters to me too. FormBlends states plainly that compounded medications are not FDA-approved, and it keeps its compounded results separate from the branded clinical-trial numbers rather than blending them together to look more impressive. For anyone planning to be on a program for months, not weeks, that kind of straight talk tells you the provider isn’t going to spring a surprise on you later. The real value being sold here isn’t the vial, it’s the screening for those label contraindications [7], the prescription, the licensed-pharmacy dispensing instead of a mystery mailer, and the follow-up.
I’d put HealthRX in the same conversation, one tier below on my list but in the same compliant category. It leads with licensed clinical oversight and dispenses supervised therapy through proper pharmacy channels rather than selling a research chemical with a warning label. The same honest caveat applies to it, compounded medications through HealthRX are not FDA-approved either, and the value again is the oversight wrapped around them. If I were choosing between the two, my actual questions would be which one is licensed in my state and whose clinical approach fits my situation, since both sit inside a recognized telehealth framework, which is the thing that matters for something you’ll be doing for months.
For the record, because you’ll run into them anyway, I also read through Pure Rawz, Core Peptides, and Biotech Peptides while researching this. I’m naming them so you recognize them if you see them, not recommending them. They sell peptides under “research use only” labeling, with no clinician, no prescription, no licensed-pharmacy dispensing, and no follow-up. Pure Rawz sells research peptides, SARMs, and nootropics under that research label. Core Peptides is a US-based research-chemical retailer that sometimes publishes its own certificates of analysis, but those are documents the company chooses to hand you, not something FDA-verified. Biotech Peptides is another research-chemical supplier with a similarly labeled catalog. None of these is a metabolic-health program. They sit outside the actual health-focused part of this search, which is why I’m not ranking them against the telehealth providers at all.
What I’d actually do
Slower, honestly. There’s an intake form, a real consultation, a prescription, and follow-up visits down the line. Ordering a vial with a research-use sticker is faster. But I went into this asking about keeping weight off and supporting my metabolism over time, not about the fastest possible checkout, and the involvement isn’t friction standing between me and the goal. It is the goal, or at least the mechanism that makes the goal possible. The quick-drop shortcut and the durable-health plan are different projects wearing similar labels, and after a week with the primary sources open in twelve browser tabs, I’m convinced the supervised route is the one actually built for the second project.
A few more things I looked up
Can a peptide alone keep weight off by itself? From everything I read, no. Even the GLP-1 medications with solid trial data work best as part of a supervised plan that also accounts for how you eat and move, which is part of why an ongoing clinical relationship matters more than the specific vial in your fridge. The compounds with the loudest metabolic marketing and the thinnest evidence, AOD-9604 [5] and MOTS-c [6], definitely will not fill that gap on their own.
Tirzepatide or semaglutide, which one actually wins for long-term metabolic health? Both are backed by real evidence, so this isn’t a case of one being legitimate and one being snake oil. Tirzepatide produced larger average weight loss in trials, up to roughly 20.9% at the 15 mg dose over 72 weeks [1], and works on two receptors instead of one. Which is right for you depends on tolerability, contraindications, and a clinician’s judgment over time, which is precisely the call a supervising provider exists to help make, not something I’d try to answer for myself from a spreadsheet of trial numbers.
What actually changed with the FDA in 2026? This is the part that reframed my whole search. The agency warned 30 telehealth companies over compounded-GLP-1 marketing in March 2026 [8], and separately told a research-peptide seller that “research use only” didn’t exempt its retatrutide and tirzepatide from being treated as unapproved new drugs [9]. If I take one lesson from digging through both of those, it’s to pick a provider standing on solid legal ground, not one leaning on a disclaimer that the FDA itself has already pushed back on.
How I actually approached this
This isn’t a scored ranking, it’s a buyer’s-guide-style dig through the evidence, done the way I do most of my research: read the primary source, note what it actually says, and don’t let a company’s own copy stand in for that. I judged the compounds on whether real human evidence backs them for weight (proven for the GLP-1 medications, investigational for retatrutide, thin or nonexistent for AOD-9604 and MOTS-c). I judged the providers on the things that matter for an ongoing supervised program: clinician evaluation and continuity, licensed-pharmacy dispensing, honesty about approval status, follow-up support, and whether the whole operation sits inside a recognized legal framework. I didn’t weigh price or shipping speed, because neither one tells you whether a program will actually support you safely for months. And I didn’t rank the research-chemical retailers against the telehealth providers, because they’re not playing the same game, and their relative purity isn’t something I can verify from my desk anyway.
What are peptides for weight loss, and how do they actually work?
Peptides for weight loss are short chains of amino acids that signal specific processes in the body, most often the hormones that control hunger, insulin response, and fat metabolism. The ones actually used clinically, semaglutide and tirzepatide, mimic gut hormones called incretins that slow gastric emptying and reduce appetite. They’re not stimulant-style fat burners. From what I read, they work by turning up the volume on your body’s own satiety signals rather than introducing something foreign to the system.
Are peptides safe for weight loss, or is the risk overstated?
FDA-approved peptides used under medical supervision have a documented safety profile from large clinical trials, though side effects like nausea, vomiting, and in rarer cases pancreatitis are real and worth a direct conversation with a physician. The bigger risk I found sits in the unregulated market, where products sold online with no oversight carry no guaranteed purity or dosing accuracy. A supervised program cuts that risk substantially, because someone is actually monitoring labs, adjusting doses, and screening for contraindications before you ever start.
What is the best peptide for weight loss, and does it depend on your health history?
There isn’t one best peptide for everyone, and I’d treat any program that skips your health history before recommending one as a warning sign. Tirzepatide currently shows the strongest average weight-loss outcomes in published trials, but semaglutide may fit someone with a particular cardiovascular profile better, and older compounded peptides like CJC-1295 or ipamorelin have much thinner clinical evidence behind them overall. A physician actually reviewing your labs, medications, and goals is what determines the right answer, not a generic ranking.
Where should you actually buy peptides for weight loss without getting burned?
Buy through a licensed medical provider or a physician-supervised compounding pharmacy, not a research-chemical site or a supplement storefront. Compounding pharmacies operating under state board oversight and USP standards, the model FormBlends uses, hand you a tested, labeled product with a prescribing clinician actually in the loop. Anything marketed “for research use only” is not intended for human use under current FDA guidance, and using it anyway puts both the quality and the legality squarely on you.
References
- Tirzepatide once weekly for the treatment of obesity (SURMOUNT-1): mean weight change −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) vs −3.1% placebo at 72 weeks. New England Journal of Medicine, 2022. https://pubmed.ncbi.nlm.nih.gov/35658024/
- Triple-hormone-receptor agonist retatrutide for obesity, Phase 2 (Jastreboff et al.): −17.5% at 24 weeks and −24.2% at 48 weeks (12 mg) vs ~2% placebo. New England Journal of Medicine, 2023. https://pubmed.ncbi.nlm.nih.gov/37366315/
- Retatrutide Phase 3 TRIUMPH-1: 12 mg dose −28.3% average body weight at 80 weeks vs −2.2% placebo. Eli Lilly, May 21, 2026.
- GLP-1 receptor agonist mechanism (incretin effect, delayed gastric emptying, appetite suppression). StatPearls, NCBI Bookshelf.
- Safety and tolerability of the hexadecapeptide AOD9604 in humans (Stier, Vos, Kenley): well tolerated, profile indistinguishable from placebo. Journal of Endocrinology and Metabolism, 2013. (Honest context: AOD-9604 was discontinued as an obesity drug after a larger 24-week trial showed no significant weight loss vs placebo.)
- Effect of aerobic and resistance exercise on the mitochondrial peptide MOTS-c in breast cancer survivors: exercise raises endogenous MOTS-c. Scientific Reports, 2021. (Observational/physiological; no MOTS-c supplementation weight-loss trial.)
- Semaglutide (Wegovy) prescribing information: boxed warning for thyroid C-cell tumors; contraindicated with personal or family history of medullary thyroid carcinoma or MEN 2. DailyMed.
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1 products. FDA press announcement, March 3, 2026.
- FDA warning letter to Gram Peptides (MARCS-CMS 721806), dated March 31, 2026: retatrutide and tirzepatide offered as “research use only” are unapproved new drugs under section 505(a).
Written by Greta Delgado, freelance health reporter. Working from the primary literature cited above. Last reviewed February 2026.
For general awareness only. Decisions about medication belong with you and your clinician.

